
Some people who suspect they have Morgellons may be right. Some may be dealing with something else entirely. Others may have overlapping problems: real skin findings, real sensations, real suffering, and an explanation that still needs to be sorted out carefully.
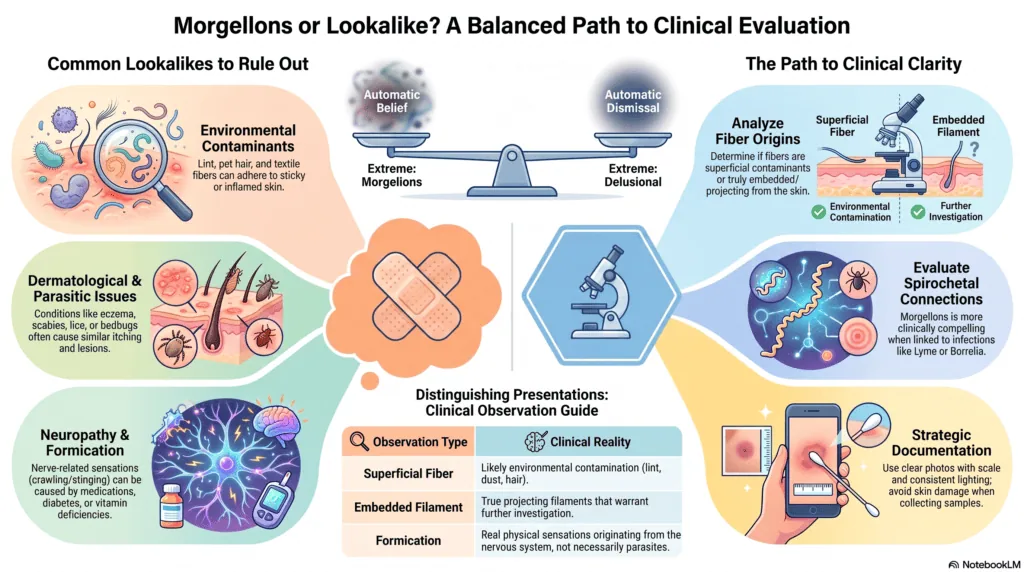
That is why this page exists. Not every fiber, particle, itch, lesion, crawling sensation, or strange image under magnification proves Morgellons. But “delusional infestation” should not become a shortcut label either. Patients deserve evaluation, not automatic belief and not automatic dismissal.
The responsible approach is simple: rule things in or out step by step. That means considering common skin conditions, real infestations, environmental contamination, neuropathy, medication effects, metabolic issues, psychiatric contributors, infections, and true embedded or projecting filaments before deciding what is happening.
Morgellons patients are often caught between two extremes. One side says every unexplained skin symptom is Morgellons. The other side says every report of fibers or crawling sensations is delusional. Both approaches can hurt patients. The truth is usually more complicated, and the evaluation should be more careful.
Why This Page Matters
Misidentifying symptoms can cause real harm. A person who mistakes scabies, dermatitis, neuropathy, medication side effects, wound irritation, or environmental fibers for Morgellons may spend months chasing the wrong explanation. They may over-clean, pick at skin, use harsh chemicals, buy expensive protocols, or become more frightened by online content.
But the opposite mistake is also dangerous. A clinician who immediately assumes delusion without examining lesions, reviewing photos, considering infections, analyzing fibers, or ruling out other causes may miss treatable disease. Patients can be wrong about a theory and still be right that something is happening.
The goal is not to prove every patient has Morgellons. The goal is to protect patients from both misdiagnosis and dismissal.
Symptoms Can Be Real Even When the Explanation Is Wrong
A person can feel crawling, burning, stinging, itching, biting, or movement sensations and still not know the cause. A person can find fibers, lint, pet hair, textile material, wound debris, or particles on the skin and misinterpret what they mean. A person can have lesions and still need a careful dermatologic workup before deciding whether those lesions fit Morgellons, dermatitis, infection, scratching, infestation, allergy, or another condition.
This distinction matters. Being mistaken is not the same as being delusional. Having a delusional belief is not the same as being “bad” or “crazy.” And having Morgellons-like symptoms does not mean every online explanation is safe or accurate.
Patients deserve language that is careful enough to protect them and respectful enough to keep them engaged in care.
Morgellons Should Be Ruled Out, Not Assumed Away
One of the biggest mistakes in the Morgellons conversation is treating the diagnosis as if there are only two choices: either every patient who suspects Morgellons is correct, or every patient is delusional. Real life is more complicated than that.
Some people who believe they have Morgellons may be dealing with another condition entirely. Others may have real skin findings, fibers, lesions, neuropathic sensations, tick-borne illness history, or overlapping medical issues that deserve closer examination. The responsible approach is not automatic belief and not automatic dismissal. The responsible approach is to rule things in or out step by step.
This matters because “delusional infestation” should not become a shortcut label for patients who report crawling sensations, fibers, particles, or skin lesions. A patient bringing samples, photographs, or observations to a clinician is not automatically delusional. Sometimes the sample may be lint, dust, textile fiber, pet hair, wound debris, or environmental contamination. Sometimes the sensation may come from neuropathy, medication effects, anxiety, substance exposure, skin irritation, or another medical condition. Sometimes there may be true embedded or projecting filaments that deserve closer examination.
The key point is simple: Morgellons should not be assumed from every fiber, but it should also not be dismissed without looking. If visible fibers or unusual skin findings are present, they should be documented carefully and, when appropriate, examined by a qualified clinician or laboratory. If the fibers are superficial contaminants, that matters. If they are embedded or projecting from skin, that matters too.
What the Delusional Infestation Review Actually Says
The review Reframing delusional infestation: perspectives on unresolved puzzles is important because it does not support lazy dismissal. It says physicians should distinguish true observations, mistaken beliefs, overvalued ideas, and delusions on a case-by-case basis. It also says that presenting a specimen is not automatically delusional behavior.
“A diagnosis of MD is more convincing when spirochetal infection is identified.”
Reframing delusional infestation: perspectives on unresolved puzzles
That sentence is important. It does not mean every person with itching, crawling sensations, lint, dust, skin debris, or unclear magnified images has Morgellons. It also does not mean Morgellons should be dismissed before skin findings, fiber evidence, neurologic symptoms, infection history, and possible spirochetal connections have been considered.
The review gives patients and clinicians a practical middle ground: do not self-diagnose Morgellons from internet photos or loose fibers, but do not jump straight to a psychiatric label before evaluating the evidence.
The Spirochete Question: When Morgellons Becomes Harder to Dismiss
Morgellons becomes more clinically compelling when compatible skin findings are accompanied by evidence of spirochetal infection. That may include evaluation for Lyme disease, relapsing fever Borrelia, syphilis, or other spirochetal infections when history, symptoms, exposure, and clinical judgment support testing.
This does not mean a positive history of tick exposure proves Morgellons. It does not mean every negative test rules out every possibility. It means the question should be taken seriously enough to evaluate carefully.
A responsible workup should ask: Are the fibers superficial contaminants or embedded/projecting from skin? Are lesions primary or caused by scratching? Are there signs of infection? Is there eczema, dermatitis, scabies, lice, bedbugs, allergy, neuropathy, medication effects, substance exposure, metabolic illness, vitamin deficiency, or another explanation? Is there a history of tick exposure, Lyme disease, syphilis, or another spirochetal infection that should be evaluated?
This is the middle ground patients need. Morgellons should not be self-diagnosed from internet images or loose fibers. But it also should not be assumed away with a psychiatric label before the skin findings, neurologic symptoms, infection history, and possible spirochetal connections have been considered.
Common Reasons Someone Might Mistakenly Believe They Have Morgellons
The following conditions and situations can sometimes be mistaken for Morgellons or contribute to Morgellons-like symptoms. This list is not meant to diagnose anyone. It is meant to help patients and clinicians avoid skipping obvious possibilities.
Environmental Fibers, Lint, Pet Hair, and Textile Material
Loose fibers are everywhere: clothing, bedding, towels, carpets, furniture, pets, bandages, dust, wound dressings, and the air. When skin is sticky, inflamed, moist, broken, or covered with ointment, environmental fibers can adhere to lesions and look alarming.
Finding fibers on the skin does not automatically prove Morgellons. The more important question is whether fibers are superficial contaminants or truly embedded in or projecting from skin in a hair-like manner. That distinction requires careful documentation and, when possible, professional evaluation.
Dermatitis, Eczema, Allergies, and Irritated Skin
Inflamed skin can itch, burn, crack, ooze, bleed, sting, and heal slowly. Eczema, contact dermatitis, allergic reactions, dry skin, irritants, soaps, topical products, adhesive bandages, cleaning chemicals, and environmental exposures can all create confusing skin symptoms.
When skin is inflamed, scratching or rubbing can make symptoms worse. This can create a cycle where the original problem becomes harder to identify because the skin has been repeatedly irritated or injured.
Scabies, Mites, Lice, Bedbugs, and Other Infestations
Real infestations can occur and should be ruled out when symptoms fit. Scabies can cause intense itching, especially at night, and may cause a pimple-like rash or tiny burrows. Lice, bedbugs, fleas, mites, and other exposures may also cause itching, bites, rashes, or anxiety about infestation.
If multiple people in a household are itching, if symptoms are worse at night, if there are bite-like lesions, if travel or exposure history fits, or if there are visible insects or mites, a clinician or qualified pest professional may need to evaluate the situation. Do not assume every crawling sensation is Morgellons, but do not assume every patient is imagining infestation either.
Learn more from the CDC’s scabies information page: About Scabies.
Neuropathy, Paresthesia, and Formication
Crawling, tingling, burning, buzzing, prickling, or “bugs under the skin” sensations can come from nerve-related causes. This type of sensation is sometimes called formication. It can be associated with neurologic conditions, medications, substance exposure or withdrawal, anxiety, metabolic problems, menopause, vitamin deficiencies, diabetes, thyroid disease, and other medical issues.
Formication can feel extremely real because the sensation is real to the person experiencing it. The question is not whether the patient feels it. The question is what is causing it.
Learn more from Cleveland Clinic’s overview of formication: Tactile Hallucinations/Formication.
Medication Effects, Substance Exposure, and Withdrawal
Some medications, stimulants, recreational drugs, withdrawal states, and chemical exposures can contribute to itching, crawling sensations, anxiety, skin picking, insomnia, or unusual body sensations. Patients may not connect these symptoms with medications or exposures unless a clinician asks carefully.
This does not mean the patient is “making it up.” It means the body and nervous system can produce distressing sensations for many reasons. A medication and exposure review can be an important part of the workup.
Skin Picking, Over-Cleaning, and Harsh Topical Routines
Even when the original symptom is real, aggressive routines can make the situation worse. Digging, scraping, squeezing, repeated tape stripping, bleach, peroxide overuse, harsh cleaners, excessive bathing, abrasive exfoliation, and strong topical products can injure skin and create new lesions.
This can make documentation harder because clinicians may see secondary damage rather than the original problem. Harm reduction matters: protect the skin, photograph before disturbing lesions, and avoid routines that create new wounds.
Delusional Infestation, Handled Carefully
Delusional infestation, sometimes called delusional parasitosis, is a real diagnosis. Mayo Clinic describes it as a condition where a person firmly believes they are infested despite physical examination not supporting that belief. But this diagnosis should not be thrown at patients casually or used as an insult.
A careful clinician should first consider whether the patient’s observations are true, mistaken, overvalued, or delusional. Real infestations, skin disease, neurologic symptoms, metabolic illness, vitamin deficiencies, medication effects, substance exposure, infection, and other contributors should be considered before primary delusional infestation is diagnosed.
Learn more from Mayo Clinic’s overview: Delusional Parasitosis.
Signs That Deserve Prompt Medical Attention
Some symptoms should not be managed through internet research alone. Seek medical care promptly if you have:
- rapidly worsening wounds or spreading redness
- warmth, swelling, pus, red streaking, fever, or signs of infection
- severe pain, numbness, weakness, confusion, or new neurological symptoms
- lesions near the eyes, genitals, or other sensitive areas
- symptoms affecting multiple household members
- severe insomnia, panic, hopelessness, or thoughts of self-harm
- skin damage from harsh chemicals, digging, scraping, or burning
If you feel at risk of harming yourself or someone else, seek emergency help immediately. Morgellons-related distress can become overwhelming, and getting urgent support is a safety step, not a failure.
How to Document Symptoms Without Making Things Worse
Good documentation can help patients. Panic documentation can hurt them. The goal is to preserve useful evidence without damaging skin or creating confusing artifacts.
- Photograph before touching. Take clear photos before cleaning, picking, squeezing, scraping, or applying products.
- Use consistent lighting. Natural light or the same indoor lighting is better than dramatic lighting that changes color and shadows.
- Include scale. Use a ruler, coin, or other reference object when photographing lesions.
- Keep a timeline. Write down when symptoms started, what changed, what helped, and what worsened symptoms.
- Save samples carefully. If collecting a fiber or particle, use clean materials and label the date, body location, and whether it was loose, attached, embedded, or projecting.
- Avoid over-magnification. Extremely magnified unclear images can create more confusion than clarity.
- Do not injure skin for evidence. Digging for samples can create secondary wounds and weaken your case.
For a more detailed guide, see: How to Document Morgellons Symptoms and Fibers.
How to Talk to a Doctor Without Getting Immediately Dismissed
It is unfair that patients have to think strategically about how to present symptoms, but many Morgellons patients have learned that presentation matters. A calm, organized appointment is more likely to lead to examination than a large collection of theories, videos, or unclear images.
Bring a concise timeline. Bring a few clear photos. Bring a short symptom list. Bring medication and exposure history. Bring any relevant tick bite, rash, Lyme disease, syphilis, or infection history. If fibers are present, describe whether they were loose, stuck to ointment, embedded, or projecting from skin.
Instead of demanding that a doctor agree with a diagnosis, consider asking:
- Can you examine the lesions and document what you see?
- Do these lesions look primary, infected, allergic, irritated, or caused by scratching?
- Should scabies, lice, bedbugs, mites, dermatitis, eczema, allergy, or infection be ruled out?
- Could neuropathy, medication effects, diabetes, thyroid disease, vitamin deficiency, or another condition explain the sensations?
- If fibers are present, can they be examined or referred for appropriate analysis?
- Based on my history, is testing for Lyme disease, syphilis, or another spirochetal infection appropriate?
- Would a dermatology referral, biopsy, culture, or infectious disease evaluation be reasonable?
This approach does not guarantee a good appointment. But it makes it harder for the visit to become a debate over internet theories and easier for the clinician to focus on observable findings.
What Clinicians Should Not Skip
For clinicians, the most important point is this: a patient reporting fibers, crawling sensations, or infestation concerns should not automatically be dismissed. A careful evaluation should separate observation from interpretation.
A patient may truly observe fibers but misidentify them. A patient may have textile contamination stuck to lesions. A patient may have real neuropathic sensations. A patient may have real infestation. A patient may have dermatitis, infection, scratching, or medication-related symptoms. A patient may also have embedded or projecting filaments and a history that warrants consideration of Morgellons and spirochetal infection.
When clinicians skip the evaluation and jump straight to a psychiatric label, patients often disappear into online communities where fear-based claims and unsafe advice are waiting. Careful examination is not just medically appropriate. It is harm reduction.
What This Page Is Not Saying
This page is not saying Morgellons is fake. It is not saying patients should stop looking for answers. It is not saying every person with crawling sensations is delusional. It is not saying every doctor understands Morgellons. It is not saying every negative test ends the discussion.
It is saying that not every suspected case is Morgellons, and patients are safer when common lookalikes are ruled out. It is also saying that Morgellons should not be dismissed before skin findings, fibers, symptoms, infection history, and possible spirochetal connections have been considered.
Patients can misinterpret symptoms. Doctors can dismiss too quickly. Both problems hurt people.
Where to Go Next
If you are unsure whether you have Morgellons, the next step is not panic. The next step is careful documentation, medical evaluation, and a willingness to rule out other causes without accepting dismissal.
- Learn how to document Morgellons symptoms and fibers
- Find a doctor familiar with Morgellons and related conditions
- Read Morgellons research papers and studies
- Read about the exploitation of Morgellons
- Explore books and patient resources for Morgellons
- Take the Morgellons Survey
References and Resources
- Reframing delusional infestation: perspectives on unresolved puzzles
- CDC: About Scabies
- Cleveland Clinic: Formication
- Mayo Clinic: Delusional Parasitosis
Medical and Safety Disclaimer
This page is for education and patient advocacy only. It is not medical advice, diagnosis, or treatment guidance. If you have worsening wounds, signs of infection, fever, severe pain, neurological symptoms, mental health crisis symptoms, or urgent health concerns, seek care from a qualified medical professional or emergency service.
Summary
Not every suspected case is Morgellons. Some people may be dealing with dermatitis, scabies, environmental fibers, neuropathy, medication effects, substance exposure, infection, skin picking, or another explanation. Those possibilities should be taken seriously.
But Morgellons should not be dismissed without looking. The more responsible path is to evaluate fibers, examine lesions, consider common lookalikes, review neurologic and infection history, and remember that a Morgellons diagnosis becomes more convincing when spirochetal infection is identified.
Patients deserve neither blind validation nor automatic dismissal. They deserve careful evaluation.
